Practice Management Basics
No clinician, whether in private practice, academia, or other models, can care for patients in the long run if the practice runs red. Further, understanding business principles can help clinicians work smarter not harder, can empower them, and may help reduce burnout. In the context of a private practice or employed model, clinicians may oversee or partner with their business administrators to review the following tools and “vital signs” of the practice.
What is benchmarking, and why should I care?
Benchmarking is critical on a personal basis to assess the market value of a clinician’s salaries, work effort, and other benefits. At a practice level, it can help 1) understand the practice’s financial strengths and weaknesses to increase profitability and efficiency, 2) provide mechanisms to compare a practice to peers and explore tools available to assist with this process, 3) determine practice deliverables to assess ongoing integrity/trends of the practice’s productivity, revenues, and expenses, 4) improve opportunities to set goals for improvements, and 4) promote buy-in from all levels of organization on need for change, if indicated. Consequently, with appropriate benchmark data, whether internal or externally derived, the data may also be leveraged to negotiate contracts with employers, commercial payers, or other stakeholders.
In order to benchmark within a practice, the practice must have the ability to understand its processes and generate relevant reports. We will cover a few critical areas:
The Master Fee schedule
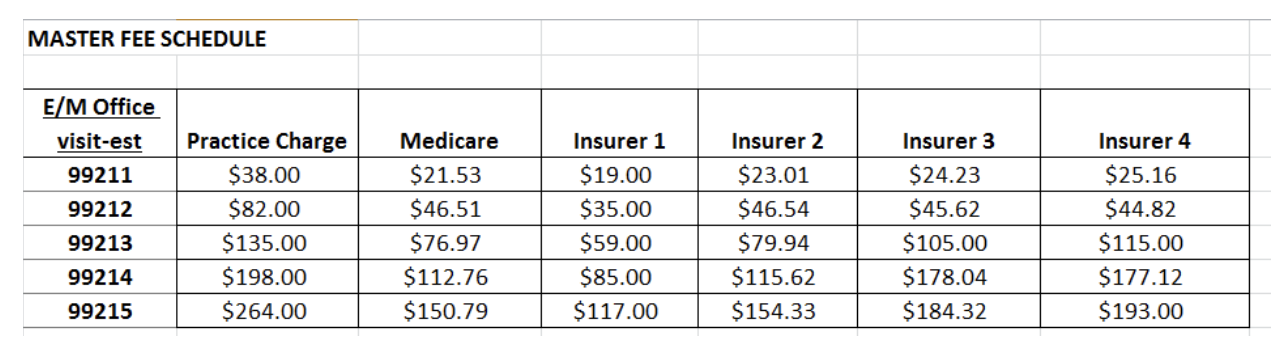
When a practice contracts with an insurance carrier, the practice agrees the insurance carrier will pay the practice a set fee for CPT codes performed. Payment rates will often be different for each insurer. Further, the clinician (practice) must also be aware that insurance contracts stipulate the payer will pay the lesser of two rates: the charge rate by the practice, or the negotiated payment rate by the insurance carrier. Thus, a practice must track all relevant CPT codes, practice charge rates per CPT, and the reimbursement rates per CPT per insurance carrier.
This spreadsheet is critical to every practice for number of reasons. First, if the charge rate is below the negotiated rate an insurance carrier is willing to pay, the practice is giving money away. By simply increasing the charge rate to equal or exceed the negotiated rate, the practice will generate additional income. This is the lowest hanging fruit. Of note, it is not uncommon to set the charge rates at about 125-150% of the highest negotiated payment rate to ensure the practice does not make the same mistake if the rates were to change the following year. Second, this spreadsheet will allow the practice to intermittently audit and verify that the insurance carrier is paying the contracted rate to the practice. Third, knowing this dollar value upfront allows the front desk to collect any coinsurance or percent of the cost of the visits that the patient may be financially liable. Lastly, the practice can determine if the negotiated rate by an insurance carrier is at market value, based on comparing other contracted insurance carriers noted on the table. If a carrier’s rates are below the market value, this can prompt the practice to communicate with the insurance carrier to discuss if the negotiated rate can more closely match the market value based on the benchmark data now available from the other insurance carriers.
Example of a master fee schedule:
1. Revenue Cycle
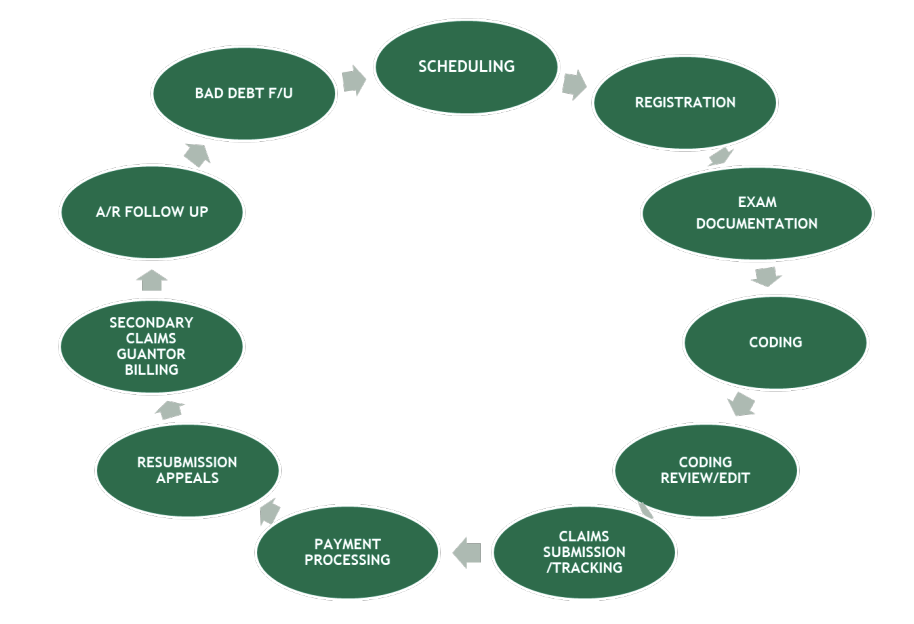
The revenue cycle includes all the steps of the patient visit from clinical care and financial remuneration. Within each step of this cycle, there are a number of measures that can be benchmarked to ensure the practice is financially viable. For instance, at the time of scheduling, a patient’s insurance must be vetted. If the practice does not take this particular insurance, the conversation would need to be adjusted accordingly. A follow-up call is generally made prior to the visit to reaffirm the patient’s appointment time, date, and location (if applicable), as well as insurance. Vetting insurance is one the most important steps to consider in the revenue cycle. At the time of Registration, all copayments and deductibles should be paid. There should not be a need for the practice to send a bill to the patient for future monies owed due to the diminished probability of collecting, in addition to the financial costs associated with sending a bill. Thus, an important benchmark is 98% of co-pay, coinsurance and deductibles should be collected at the time of the visit. While the following bubbles of Exam documentation and Coding are components of the clinical visit, it is standard that a visit note is closed and available to bill within 48 hours. Reasons this is important is to help the billing department track unprocessed claims as well as the risk of not getting paid for the claim at all. Specifically, a contract clause typically exists such that if a practice does not submit a claim within a certain period of time, the carrier is no longer obligated to pay for the claim.
Example of a revenue cycle:
2. Accounts Receivable
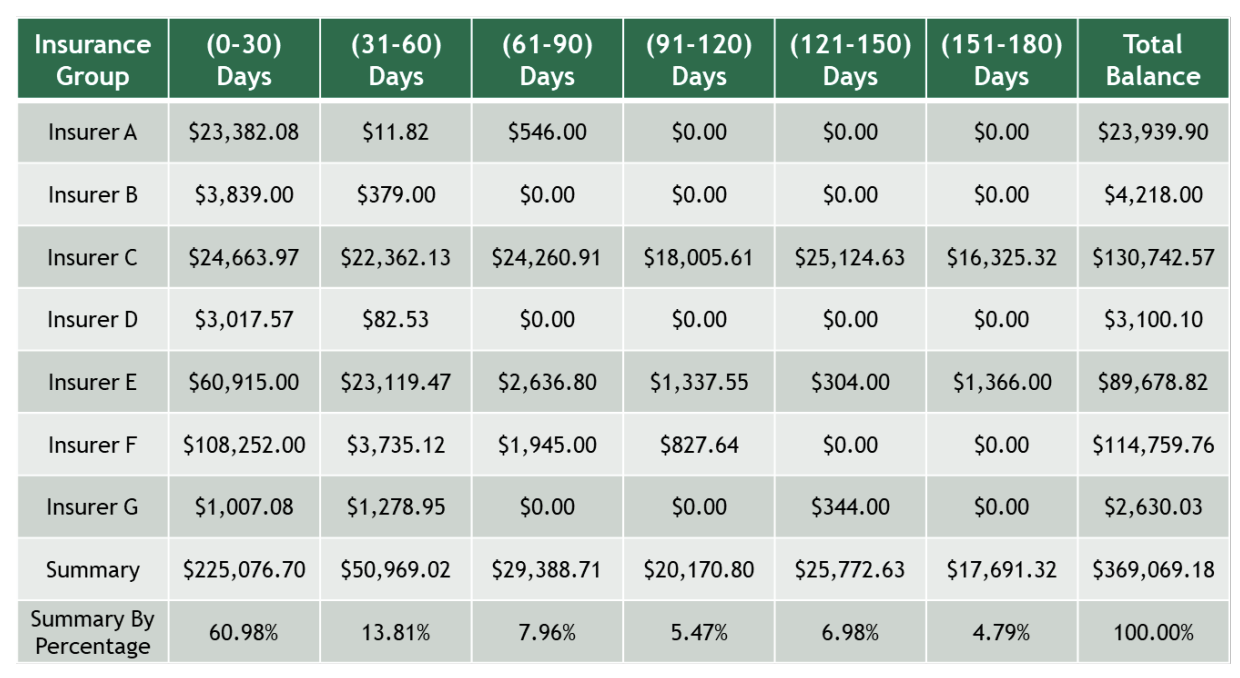
The next several steps within the revenue cycle rely on the capabilities of the billing staff of the practice. However, the assessment of A/R follow-up, or Accounts Receivable followup, is a critical step in revenue cycle management that a clinician may be involved. Accounts Receivable reflects the money that is owed to a practice. Because payments by a carrier for the clinical care provided to a patient do not occur the day of the visit, a certain amount of debt is created and tracked in “buckets of time” usually 1 to 30 days, 30 to 60 days, 60 to 90 days, and so forth. That is, if a payment is not made within 30 days the amount of money is moved (and tracked) into the next bucket of 31 to 60 days. The longer an outstanding bill exists, the less probable it is the insurance carrier will actually pay. On a monthly basis, a table can be created delineating monies owed by each insurance carrier over each period of time. While an older benchmark, one would expect that over 85% of monies owed sit within buckets less than 120 days. Most payers now pay "clean claims" in 30 days or less. Nonetheless, if a significant amount of money exists in the later buckets, it is up to the clinician and/or business administrator to take a deeper dive to understand why monies have not being collected. For instance, a particular payer may have a high denial rate because a particular procedure like nerve blocks are no longer covered and the practice was billing for it regardless. If the Accounts Receivable is high in a later bucket for multiple insurance carriers, there may be a concern with how the billing staff submits claims. In the example below, you can see Insurer C should be evaluated more closely.
Example of an accounts receivable report:
Conclusions:
The above examples provide some of the basic, core elements to affirm the viability and success of a practice. While this information may not be transparent nor available to all clinicians, and global change may be limited due to institutional protocols, the above provides a framework for financially evaluating a practice, asking the right questions, and perhaps impact change at least at the local level.